

Fukushima Medical University is located in a green, natural environment in the north of Fukushima Prefecture. The university comprises a School of Medicine based around the old Fukushima Women’s Medical School that was founded in 1944 and a School of Nursing that opened in 1998, a Graduate School, and Fukushima Medical University Hospital.
As the result of an ongoing drive for change and a desire to create a more open university, it became an independent administrative corporation in April 2006 – Fukushima Medical University. Fukushima Medical University Hospital offers 778 clinical beds and handles an average of 1,795 outpatients per day (fiscal 2007). It remains both a higher education facility and a regional centre for advanced medical technology.
Recommended White Papers
Recommended Buyers Guides
The Department of Radiology offers five FPD R/F systems (two direct conversion and three indirect conversion). A Shimadzu SONIALVISION safire II system was introduced in March 2008 as an upgrade for an existing system. A major factor in selecting this system was the wide-field (17in x 17in) FPD that permits kidney-ureter-bladder (KUB) radiography.
This paper reports on the utility and problems with the SONIALVISION safire II Slot Scan radiography application.
Long-length imaging
Long-length imaging is an essential radiography technique in the field of orthopedic surgery for the diagnosis of scoliosis and alignment measurements on the full length of the lower limbs. At this hospital, we conduct radiography with multiple IPs loaded in a long-length cassette and join the images together when reading them.
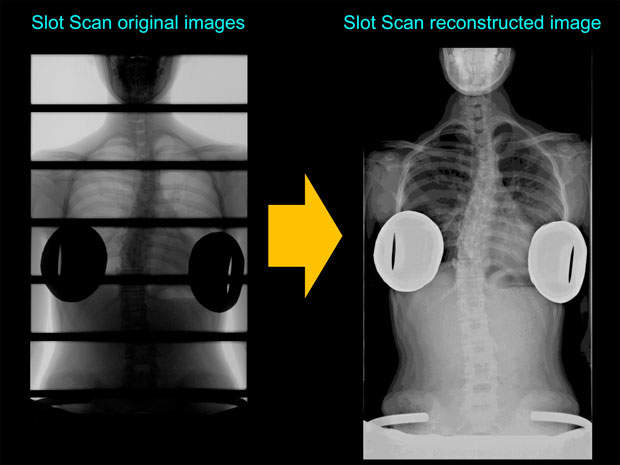
The SONIALVISION safire II system Slot Scan function conducts radiography with the X-ray beam collimated into a slit by moving the X-ray tube and FPD at constant speed in the body-axis direction and then reconstructs the information into a long-length image (Fig. 1). The radiography modes include HS (high speed) and HQ (high quality) in addition to F (frontal) and L (lateral). The radiography centre height, slot width, and speed of movement differ according to the mode. In the HS mode, the imaging chain moves at 150mm/sec and acquires data with a 6cm slot width at the radiography centre height. In the HQ mode, the imaging chain moves at 75mm/sec and acquires data with a 4cm slot width at the radiography centre height. A reference height is set to achieve appropriate image stitching during image reconstruction.
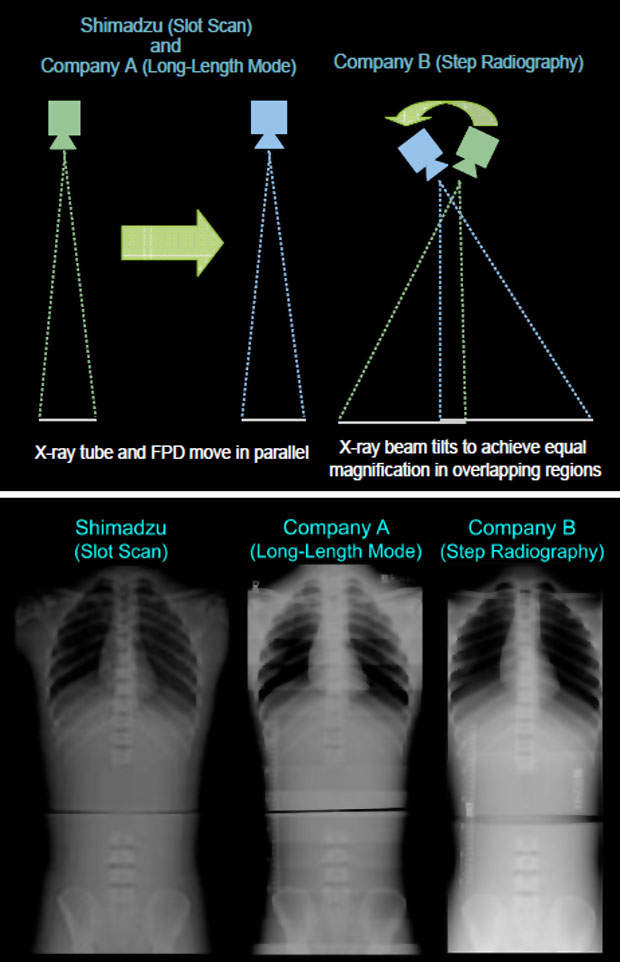
Long-length imaging is possible using FPD fluoroscopy systems from other manufacturers, in addition to the SONIALVISION safire II. The imaging method differs from manufacturer to manufacturer. Company A adopts the same parallel movement of X-ray tube and FPD used by Shimadzu, whereas Company B tilts the X-ray beam such that the magnification is identical in the overlapping regions of the two images (Fig. 2). Before we introduced the SONIALVISION safire II system, we already had instruments that offered long-length imaging functions. However, due to the complexity of setting radiography conditions and the difficulty in understanding the range of coverage, they proved inadequate to substitute for conventional cassette radiography and were not used for routine radiography examinations. However, the SONIALVISION safire II Slot Scan function is easy-to-use and frequently used for routine radiography.
Slot Scan ease-of-use
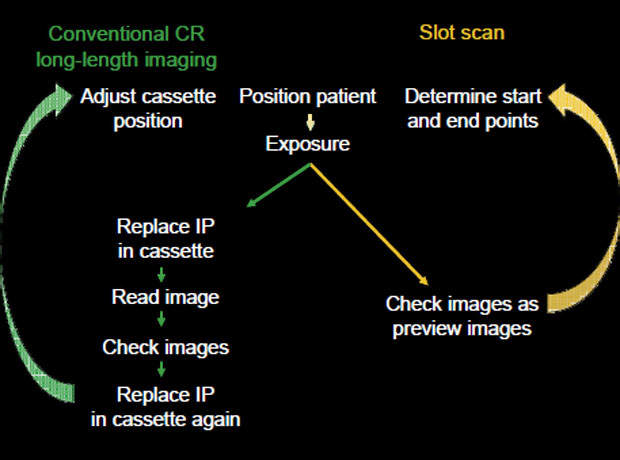
Fig. 3 shows flowcharts of the work flow for cassette radiography and Slot Scan radiography. The conventional CR long-length imaging operation is complex. It requires switching the IP and reading the image after every exposure. Patient throughput is poor, as the patient has to wait in the radiography room while the images are being checked. Conversely, Slot Scan radiography requires just the start and end positions to be set. Images can be checked immediately after radiography is complete, which reduces the examination time and improves efficiency.
Conventional CR long-length imaging is difficult for patients who have trouble standing, as it is difficult to achieve adequate SID from the table and to maintain the long imaging field. It is also difficult in cases where a wide imaging field is required, such as patients with severe scoliosis and radiography of both legs simultaneously. With its 1,400mm FPD movement range and 430mm wide coverage, Slot Scan flexibly accommodates a diverse range of radiography examinations (Fig. 4). As many scoliosis patients are young, it is important to reduce the X-ray exposure dose over follow-up examinations over many years.
Slot Scan exploits the wide dynamic range of the FPD to perform radiography with a lower X-ray exposure dose than the conventional method.
Jointly using Slot Scan and the conventional method
Long-length images are used for diagnosis of scoliosis and follow-up examinations. However, since the introduction of the SONIALVISION safire II Slot Scan, we have been concerned that the Cobb angle (that expresses the angle of curvature of the spine) obtained by Slot Scan may differ from Cobb angle from images obtained by the conventional method, because the method of linking the images differs. Slot Scan differs from the conventional method because the reference height is set above the tabletop and the overlap of the various Slot Scan images is calculated to link the images together.
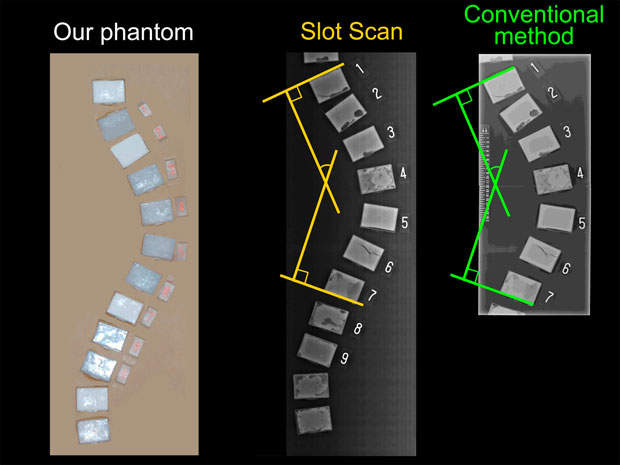
We produced a phantom to evaluate any discrepancy between the Cobb angle measured from the conventional method and from Slot Scan measurements (Fig. 5). The phantom comprised plastic cases filled with caulking that were arranged as simulated vertebrae. Measurements were performed by doctors and technologists. Both the conventional method and Slot Scan produced approximately the same measured results, confirming that no problem arises when using both Slot Scan and the conventional method.
Precautions during radiography
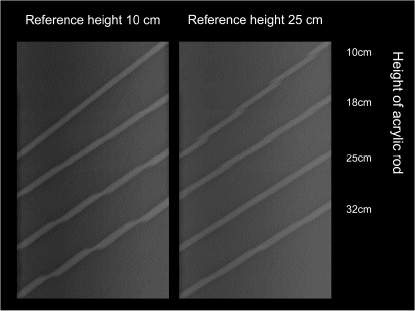
Using Slot Scan, the position of interest is adjusted to the reference height during image reconstruction to ensure accurate measurements. However, appropriate images cannot be obtained if the reference height differs from the area of interest. Fig. 6 shows Slot Scan images of acrylic rods positioned at different heights above the tabletop. The image is reconstructed correctly for the acrylic rod at the reference height. For rods higher than the reference height, the stitched positions are more separated in the reconstructed image. For rods lower than the reference height, the stitched positions are more overlapped in the reconstructed image.
Due to such artifacts at the stitched positions due to effects of the cone angle on objects at different heights from the reference height, it is important to accurately set the reference height for image reconstruction. Such effects occur readily at thicker parts of the body, such as the shoulder or pelvis. It is thought that Slot Scan reduces the effects of the cone angle by collimating the X-ray beam into a slit. However, in cases with high body thickness, such as lateral radiography of the full spine, appropriate condition settings and image reconstruction are required to further reduce these effects, such as using a combination of the longest possible SID and the HQ mode that has a narrow cone angle.
In some cases a surplus or deficiency of X-ray dose can occur in images taken with the same radiography conditions, such as at the cervical spine and other low-body-thickness regions and at the shoulder, pelvis, and other high-body-thickness regions in lateral radiography of the full spine. Ideally, radiography should be conducted with the optimal X-ray dose at each region. Differences in radiography conditions can result in unnaturalreconstructed images.
Changing the radiography conditions for each slot could produce natural-looking images to further improve the utility of this function for long-length imaging.
Conclusions
With its easy operation and excellent patient throughput, Slot Scan could replace cassette radiography. Unfortunately, as it cannot be used during other fluoroscopic examinations, it still has to be used in conjunction with the conventional method. I hope that we can use it more effectively in the future.
However, as Slot Scan operates with fixed radiography conditions, it cannot handle changes in body thickness and this can result in a surplus or deficiency of X-ray dose. This problem and the artifacts that occur at positions away from the reference height need to be resolved in the future. The Slot Scan function satisfies a range of clinical requirements and I anticipate that it will become increasingly effective for long-length imaging.
Author: Nobuhito Handa



