





Our hospital is situated on the western edge of Aichi
Prefecture. It functions as a foundation hospital for a region
not only containing the medical district of Ama and Tsushima
but also stretching as far as the western part of Nagoya City
and part of the northwest area of Mie Prefecture.
The hospital was founded in August 1943 by the Kainan
Federation Responsible for Health Care Purchasing
Cooperatives as a group hospital for local residents, with
departments of internal medicine and trauma, and 20
beds. In 1948, control of the hospital was transferred to
the Aichi Prefectural Welfare Federation of Agricultural
Cooperatives, and to this day we continue to provide
medical care based on the needs of the local community.
Recommended Buyers Guides
In February 2003, a new inpatient wing currently equipped
with 553 beds (including those in the ICU, the
convalescence / rehabilitation ward, and the palliative care
ward, and those for patients with infectious diseases) went
into operation. The Department of Radiological Technology
is situated on the first floor of the new wing. Most of our
equipment is also kept in the new wing, although we have
set up two general radiography rooms, one MDCT scanner,
and one urological system in the outpatient ward, where we
use them in the day-to-day treatment of patients.
Background to introduction of BRANSIST Safire
We used to conduct angiography with a setup consisting of
two systems: a dual-plane system (for the abdomen and
limbs) and a bi-plane system (for the head and heart)
equipped with image intensifiers. However, because of the
deterioration of the dual-plane system and a yearly increase
in the number of cardiac catheter examinations and head
examinations, we introduced Shimadzu’s BRANSIST Safire
HB9 (for the heart) bi-plane system equipped with a
direct-conversion 9in x 9in FPD, and because of the desire
of doctors to be able to observe a wide range surrounding the
region of interest in a single image, we introduced
Shimadzu’s BRANSIST Safire VC17 equipped with a
large-field direct-conversion 17in x 17in FPD.
The VC17 was the first angiography system in the world
to be equipped with a 17in x 17in FPD, and the very first
model was introduced at our hospital in August last year. I
would like to describe our experience of using it.
System overview
This system incorporates a ceiling-mounted C-arm
equipped with a 17in x 17in direct-conversion FPD, and is
capable of performing DA, DSA, RSM-DSA (Real-time
Smoothed Mask DSA), Rotational RSM-DSA (precessional
movement and pendular movement), and 3D-DSA (of the
head and abdomen). Five field sizes can be used: 17in, 15in,
12in, 9in and 6in (Table 1). The fluoroscopy and
radiography rates are shown in Table 2. Fluoroscopy rates
of 3.75, 7.5, 15, 15H, 30, and 30H can be selected.
Regarding radiography, although different times and rates
can be combined freely in accordance with the needs of the
facility, it is not possible to change the rate during an X-ray
exposure. This is one point that I think requires modification.
With Rotational RSM-DSA, precessional movement is
performed with a fixed deflection angle of 30° and a cycle
of 6s (three cycles max.), and pendular movement is
performed in a fixed range of LAO15° to RAO15°, also
with a cycle of 6s (three cycles max.). These functions
enable the three-dimensional observation of blood vessels.
The maximum rotation speed of the C-arm in 3D-DSA
when it is set behind the head is 60°/s.
Automation of aging and calibration
One superior aspect of this system is that it can
automatically perform the aging and calibration
that is required before use. With previous systems,
aging had to be performed for both fluoroscopy
and radiography by manually changing the voltage,
and it was necessary to move the C-arm to the
center position and remove the grid before
performing calibration. With this system, aging is
performed automatically when you press the start
button, and automatic calibration can be initiated
by simply checking that the SID is 110cm in the
standby position and pressing the start button. This
makes it possible to allocate more time during the
busy morning period to other tasks.
Whole-body coverage
Another advantage is that examinations can be
performed with the C-arm set behind the head, at
the right or left side, or in one of the intermediate
positions as appropriate for the circumstances or
application (Figs. 2 to 4). At our hospital,
abdominal examinations are performed with the
C-arm on the left side of the patient, with the
C-arm moved to the head to perform 3D-DSA.
Upper-extremity PTA is performed with the
patient’s arm pointing out to one side and so, in
order to make it easy for the physician to perform
the procedure, the C-arm is set behind the head. I
think that the intermediate position can be used in
head examinations, for example, when intubation
is performed on a patient with a decreased level
of consciousness and the physician needs to place objects alongside the patient’s head.
The C-arm rotation angle ranges are shown in Table 3.
Regardless of the setting position, there are no
significant restrictions on bed movement distance
and C-arm rotation and so examinations can be
performed across the entire body with few
problems.
The ceiling-mounted C-arm has a large range of
movement covering 160cm in the transverse
direction and 287cm in the longitudinal direction.
This makes it easy to handle brachial, radial and
femoral approaches, and radiography of the lower
limbs can be performed easily without having the
patient lie in the opposite direction. Incidentally, my
height is 176cm, and there is easily enough
movement to perform radiography on any area of
my body, right down to my toes. The 17in x 17in
FPD enables simultaneous radiography of both
legs, which helps save contrast medium.
Operability
The Safire-series ‘Cyber Grip’ controller enables
one-handed execution of C-arm rotation (25°/s
max.) and movement, vertical movement of the
FPD, and table movement. The ‘Direct Memory’
auto-positioning function allows angle setting and
angle registration to be performed with easy
operations. Operators have described these
features as being extremely easy to use once they
got accustomed to them.
These operations can be performed from an
operation room, from where it is possible to
support the operator.
Monitors
There are independent live and reference monitors
and images can be referred to at any time, even
during radiography or fluoroscopy, on the reference
monitor. This monitor can also be used for image
processing and measurement. Selected images
can be displayed or replayed instantly, which has
helped eliminate one source of stress during
examinations. There is also an image viewer that is
used for post-processing. Images can be
transferred to this viewer immediately after they
are obtained, allowing them to be processed while
continuing the examination. This is an extremely
convenient feature.
Safety
The system design reflects consideration of safety,
with a contact sensor on the front of the FPD and
noncontact sensors on all four sides. When we first
introduced the system, the sensitivity of the
noncontact sensors was too high, and they would
be activated, disabling C-arm operation, simply by
the operator standing. Such problems, however,
were soon resolved.
IVR shuttle
With this system, operations that were previously
performed with a mouse and keyboard, such as
switching of the fluoroscopy / radiography rate, the
selection and playback of reference images, and
image processing, can all be performed with an IVR shuttle. This makes it easy to support the
operator, and helps facilitate the smooth execution
of examinations and treatments.
SIM (super impose map)
From the time the system was first introduced, it
was possible to create map images in fluoroscopy.
To fulfill the desire to be able to perform treatment
using map images with DSA images, the system
was upgraded.
Although this function has helped to increase the
efficiency of examinations and treatments and to
reduce the consumption of contrast medium, the
procedure for creating map images from
radiography images is a little complicated, and
needs to be simplified.
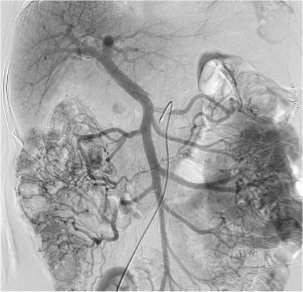
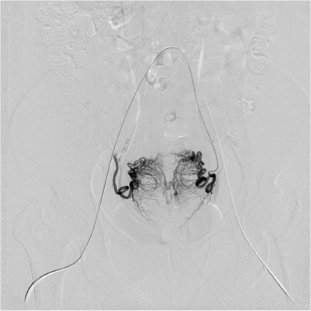
Image quality
Regarding radiographic images, not only does the
direct-conversion method give extremely sharp
images, the FPD pixel pitch of 150µm makes it
possible to obtain high-definition images that allow
even peripheral blood vessels to be observed with
ease (Figs. 5 to 7). Doctors have praised the
quality of clinical images.
Regarding fluoroscopic images, it was noted at first
that the tips of microcatheters could not be
visualized, but this problem has been resolved by
the installation of the image processing engine
SUREengine.
Summary
The large field size of this angiography system
equipped with a 17in x 17in FPD is effective for
observing both the liver and spleen at the same
time and for dealing with conditions requiring a
large field such as gastrointestinal bleeding.
On the other hand, there are some problems that
are caused by the wide FPD unit. For example,
moving the FPD too close to the patient can
obstruct the procedure. I think that such problems
can be solved, however, if technologists provide
operators with the support appropriate for the
circumstances.
This system is equipped with many functions, and
can be used effectively for the whole body.
Since introducing this system, we have gradually
had modifications and upgrades made in
accordance with our needs. There are still some
modifications that I would like to see, and I hope
that communicating these to the manufacturer will
lead to the development of an even better system.
Author: Katsutaka Hiratsuna